Draft
Please do not quote or
cite
A Survey and Report by the
Connecticut Coalition for Environmental Justice
Copyright 7/14/00 CCEJ and EBIC
This paper discusses the analytical results of a health survey conducted
in Hartford by a coalition of organized concerned citizens. We begin by
identifying the groups involved in the project and how they came to work
together. This arrangement helps to clarify the main purposes for this
research and serves as an introduction to the research model, the results,
and their importance as the basis for community based health research and
organizing.
The health survey form was designed and circulated by members of Organized
Northeasterners/Clay Hill and North End (ONE/CHANE) of Hartford under a
grant from the U.S. Environmental Protection Agency. ONE/CHANE is a neighborhood
organization based in the North End of Hartford. It is affiliated with
the Hartford Environmental Justice Network (HEJN). HEJN is a coalition
of twenty-two health and neighborhood organizations and the local affiliate
of the Connecticut Coalition for Environmental Justice (CCEJ). CCEJ is
an umbrella group for a network of grassroots activists working in urban
areas of Connecticut on local environmental issues (see Appendix II for
a descritption).
The Coalition works with regional groups such as the Toxics Action Center (TAC). It was through the course of two conferences in Connecticut and Massachusetts hosted by the TAC that the CCEJ's Dr. Mark Mitchell met and began working with Dr. Brian Lipsett of the Environmental Background Information Center (EBIC). Dr. Mitchell is President of CCEJ, a director on the Greater Hartford Hispanic Health Council, and former director of the Hartford Health Department. He has a MD from the University of Missouri and a Masters in Public Health from John's Hopkins. Brian Lipsett is organizing director of the EBIC and has a PhD in Administration of Justice from Penn State University.
Dr. Lipsett offered and Dr Mitchell formally requested EBIC's assistance
in mapping and analyzing the health survey data as a followup to the data
collection and as a preliminary step in turning the research into a component
of a broader organizing campaign in Hartford. The survey project is thus
composed of several components, but was
designed to determine if some types of health problems are concentrated
in certain neighborhoods of Hartford.
Discussion
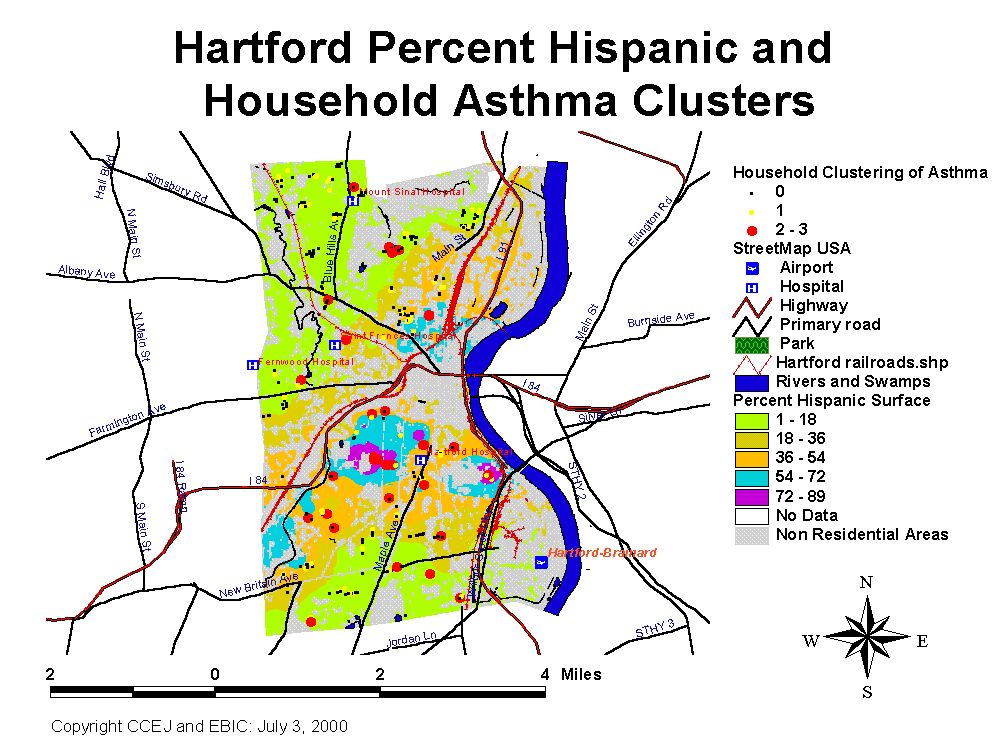
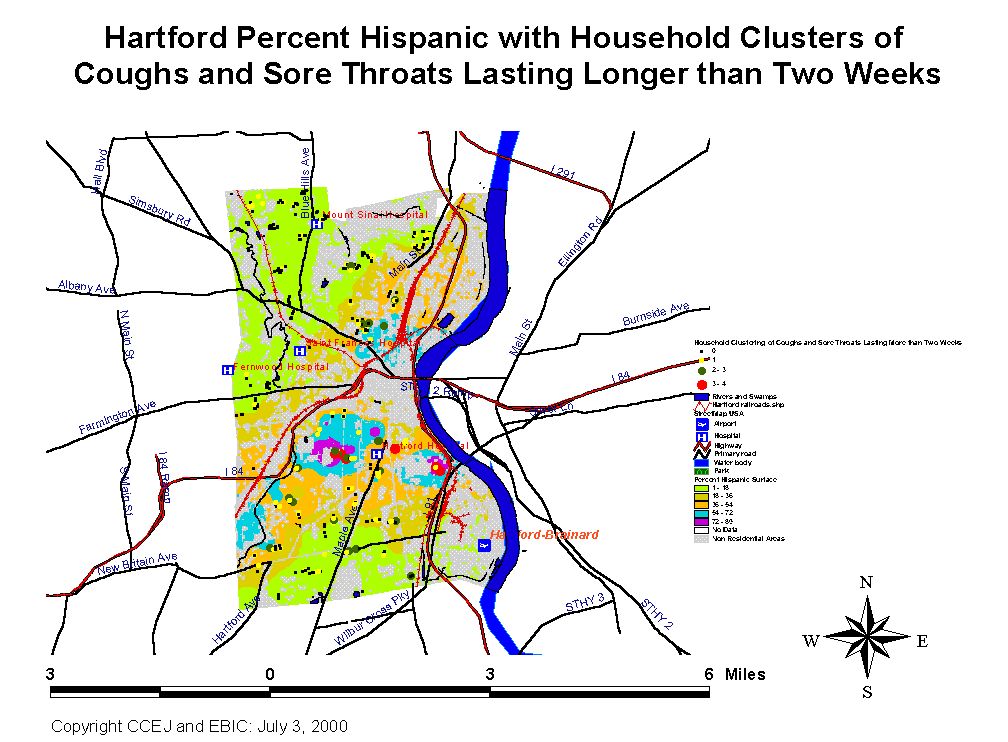
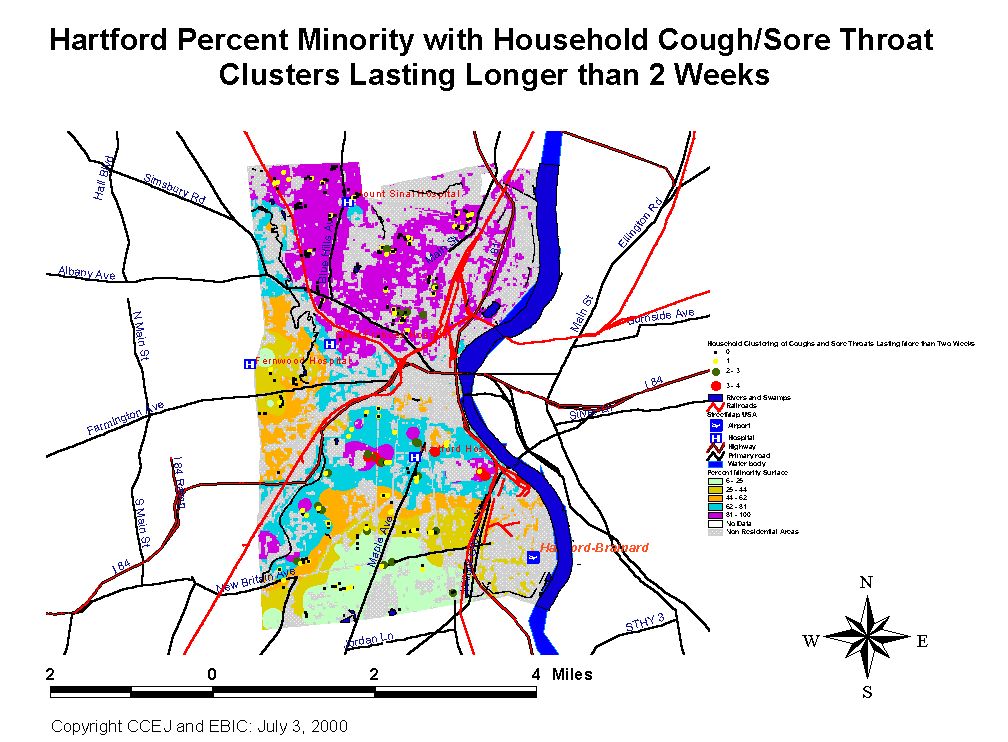
Chronic recurrent respiratory symptoms were found to be concentrated in Hispanic households. This suggests that the health risk is particularly pronounced in the southern half of the city where most of the Hispanic population lives. Further analysis is necessary but we can say for certain that there is a marked demographic pattern associated with asthma incidence in the city. These results bear out other research on the topic of asthma in Hartford. Most importantly, the relationship between asthma incidence and the incidence of coughs and sore throats needs to be further examined. Is this a new type of progressive illness and/or is it a sign of environmental stress. Certain facilities in closer proximity to these neighborhoods may be related to the problems. Other phenomenon such as housing stock may play a role. It is worth noting that the health variables we examined, particularly in our regression analysis may be multicollinear. Asthma and allergies, for example, are thought to coincide.
Methodology
A survey of certain acute
and chronic symptoms was developed with input from a committee of community
representatives, epidemiologists, health researchers and physicians based
on other published surveys and anecdotal community experience. The survey
instrument was field tested and validated. Community residents were recruited
and trained to conduct the survey in randomly selected households citywide.
Household heads answered the questionnaire for the whole household.
The survey was conducted
by volunteers who went through Hartford neighborhoods knocking on the doors
of houses and apartments in Hartford. The households were randomly selected
by dividing the city of Hartford up into 872 blocks. The sample contains
a total of 415 household survey sites. The data is derived from interviews
with 415 primary respondents who were interviewed during household visits.
A total of 1088 persons at those household sites are included in the survey.
The data was initially compiled
by Dr. Mark Mitchell. Dr. Mitchell had initial assistance from Deborah
Dumin, a Connecticut Department of Environmental Protection employee, and
Dr. Ellen Cromley, a professor of Geography at the University of Connecticut.
The survey data was then split into two separate tables, one table containing
health information for primary respondents and another table for the reported
health of other household members, based on responses from the primary
respondent.
Following survey design,
implementation and data compilation, data analysis was conducted to determine
if there were any clear geographic or demographic patterns associated with
observed health problems. The community groups involved in the survey implementation
were particularly concerned with asthma, respiratory disorders, and other
acute human ailments which may be environmentally related. The suspicion
is that there are potential clusters of these problems which may also be
associated with sources of pollution. Questions in the survey were designed
to document the occurrence and distribution of conditions of concern. In
order to do this properly, it was necessary to accurately locate the exact
positions of survey respondents households on a two dimensional surface
- a map of the city of Hartford.
This
task was accomplished by the use of Geographic Information Systems (GIS).
Health survey data was geo-coded to the household/building level and appears
on the map as point data. This approach was aided with data from the Metropolitan
District Commission Water and Sewerage Company including line data of building
footprints of structures in Hartford, street and sidewalk boundaries, interstates,
and railroads. Demographic point data for census block groups was transformed
into surface representations and was masked with the use of land use data
from the MAGIC website at the University of Connecticut (http://magic.lib.uconn.edu).
Land use data is based on analysis of satellite imagery.
Subsequent to incorporation
of the health survey data into a GIS analysis, the same data was run in
a statistics package and simple Chi Square analysis was performed. This
analysis helped to bolster findings that could be derived from a more or
less cursory visual examination of the plotted data.
Results
Dr. Mitchell and CCEJ derived
preliminary results from the analysis which showed that
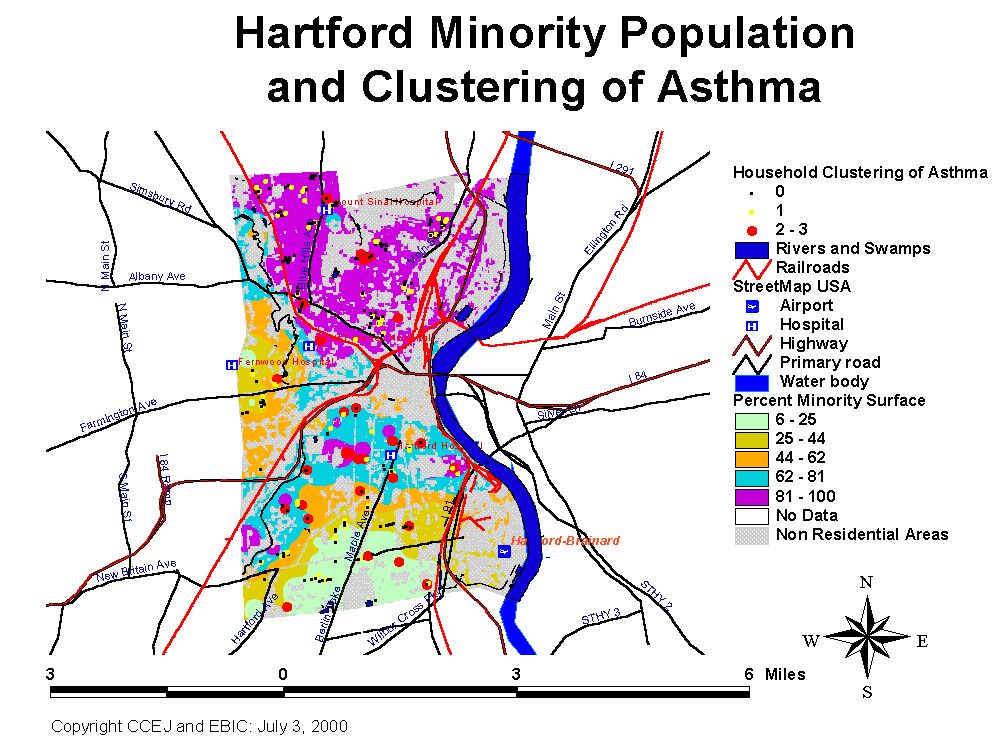
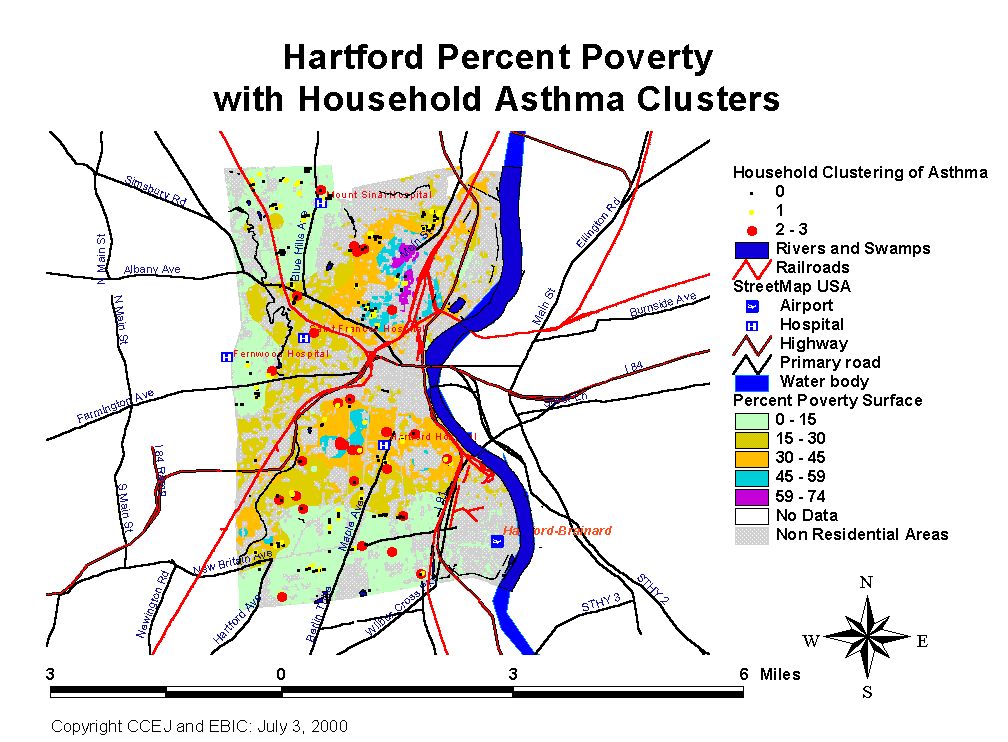
asthma is fairly evenly distributed among households throughout the city.
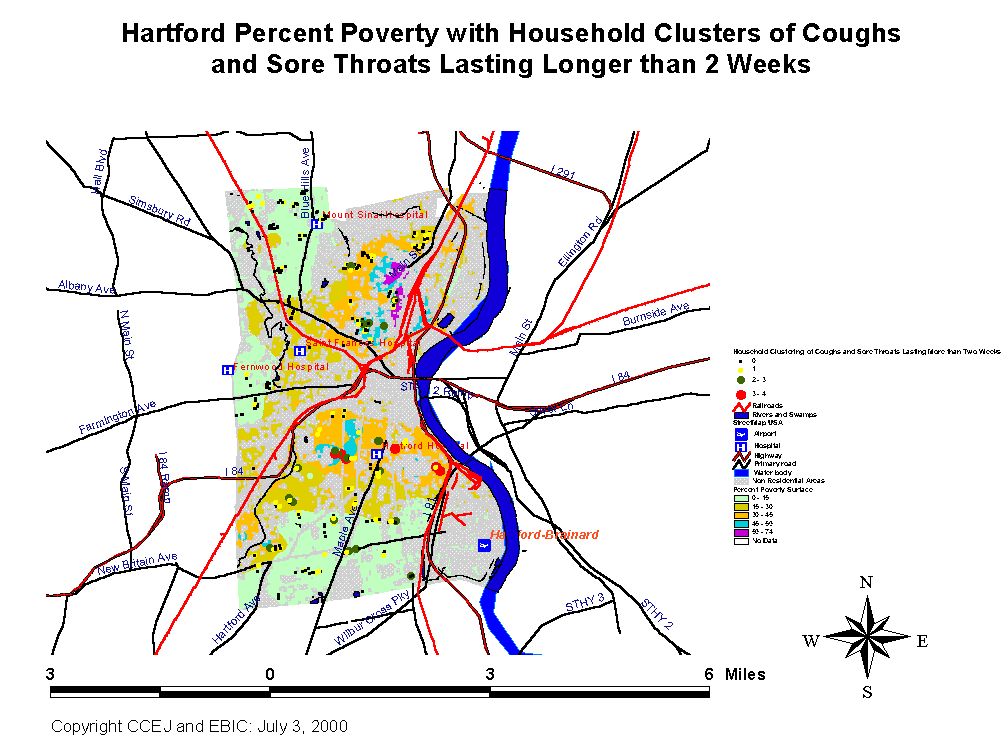
However, a preliminary analysis of cough and sore throats lasting longer
than two weeks and respiratory problems lasting longer than one month appeared
to be more common in the southern part of the city. This result is consistent
with anecdotal reports from residents that many Hartford residents get
"colds" that last for months. This is contrary to the duration of viral
upper respiratory illness (the common cold) reported in the medical literature
which is described as lasting from 4 to 10 days.
Subsequent analysis of the
data provided further support for these results and led to the observation
that the Hispanic population is more at risk for asthma, colds lasting
more than one week and other respiratory problems lasting more than one
month. We term these observed respiratory health problems of people in
Hartford as "Chronic Recurrent Respiratory Ailments (CRRA)." What follows
is a more detailed discussion of our findings.
Asthma
A sample of 1088 individuals
in 415 households was broken in two according to whether a particular record
described the reported health of a primary survey respondent or one of
673 "other" members of households. In 87 households, the primary respondent
reported asthma. An additional 30 individuals in 27 of those households
were reported to have physician diagnosed asthma. A total of 117 persons
have asthma in the 87 households where primary respondent has asthma. 2
Households were missing data in the asthma category for the primary respondent.
In addition, there were 326 households where the primary respondent reported
no asthma. Fifty other people in 41 of these households were reported to
have physician diagnosed asthma. A total of 7 individuals in 7 households
have missing data in the asthma category (2 primary respondents and 5 "other").
Table
1: CRRA in Hartford
| # of Persons | # Households | # of Housholds with Multiple Victims | # of Households with Single Victim | |
| Primary
Respondents with Asthma
(of 413 with 2 missing cases) |
87 (21) | 87 (21) | na | na |
| Number
of Other Persons
with Asthma in households where primary resp. reports Asthma (of 154 persons in 87 household with one missing case) |
30 (19.5) | 27 (31) | na | na |
| Other Members with Asthma in households where primary resp. doesn't report Asthma (of 518 persons in 326 households with 4 missing) | 50 (9.7) | 41 (12.6) | na | na |
| Asthma Totals (%) (of 1081 persons with 9 missing in 413 households with 2 missing) | 167 (15.4) | 128 (31) | 35 (8.5) | 93 (22.5) |
| Primary
Resp. with Colds or Sore Throats Lasting More than 1 Week
(of 412 with 3 missing) |
88 (21.4) | 88 (21.4) | na | na |
| Other Members with Cold/Sore Throat Lasting More than 1 week where primary resp. reports same (of 171persons in 88 households with 4 missing cases) | 31 (18.1) | 21 (23.9) | na | na |
| Other Members with Cold/Sore Throat Lasting More than 1 week where primary resp. doesn't report same affliction (of 501 persons with 7 missing in 324 households with 3 missing) | 47 (9.4) | 36 (11.1) | na | na |
| Cough/ Sore Throat Totals (%) (of 1081 persons with 7 missing in 412 households with 3 missing) | 165 (15.3) | 123 (29.9) | 28 (6.8) | 95 (23.1) |
| Primary Respondent with Allergies (of 413 with 2 missing) | 115 (27.9) | 115 (27.9) | na | na |
| Other Household Members with Allergies in households where primary resp. reports allergies (of 189 persons in 115 households) | 31 (16.4) | 22 (19.1) | na | na |
| Allergies in households where primary resp. does not report allergies (of 482 persons in 298 households | 39 (8.1) | 34 (11.4) | na | na |
| Allergy Totals (%) (of 1081 persons with seven missing in 413 households with missing) | 185 (17.1) | 149 (36.1) | 27 (6.5) | 122 (29.5) |
| Primary Resp. with Respiratory Problems Lasting more than one Month (of 415) | 29 | 29 | na | na |
Overall 128 households report
asthma in one or more members. Those households contain 167 persons who
have physician diagnosed asthma 31% (128/413) of households sampled have
one or more cases of diagnosed asthma. 15.4% (167/1081) of all persons
in 415 households have physician diagnosed asthma. 38 households have more
than one asthma sufferer. That is 9.2% of the overall household sample
and 30% of households with asthma.
Asthma and Gender
There were 295 females and 118 males acting as primary respondents. Three hundred and eleven females and 357 males were found among the other members. A total of 5 records were missing gender descriptors. Thus a total of 606 (56%) females and 475 (44%) males were in the sample. A total of 64 males out of 471 (13.6%) and 103 females out of 605 (17%) have asthma. Thus woman were more likely than men to have asthma, although the difference is statistically significant at better than the .01 level for primary household respondents only.
Age and Asthma
Amongst primary respondents,
only 2 were under the age of 18. One of these reported having asthma. (Edit
this expression "had asthma" and add percentages) There were 89 people
who were between the ages of 18-29. Twenty three of these people had asthma.
There were 130 people between 30-44, 24 of which had asthma. Likewise there
were 130 people between age 45-65. Thirty had asthma. Finally, 64 people
were over 65. Nine had asthma. Amongst other household members, there were
350 people under age 18. Fifty-five had asthma. There were 94 people were
between 18-29. Eight had asthma. There were 103 people between 30-44. Eight
had asthma. Amongst the 78 other members between 45-65, 5 had asthma. Twenty
nine other people were over 65, with only 2 having asthma. Nineteen cases
were missing data on age, two cases of which have asthma.
Asthma Concentrations
Asthma appears to be concentrated
in particular households. Ninety three households had one member with reported
asthma. An additional 35 households contain an 74 more persons with reported
asthma. That means that 8.4% of all households in the sample contain 44.3%
of all reported asthmatics while an additional 22.4% of all households
contain the remaining 65.7% of all reported asthmatics. This phenomenon
holds consistent for other respiratory tract ailments.
Coughing, Sore Throats and Other Respiratory Ailments
Twenty nine primary respondents
reported having respiratory problems that lasted more than 1 month. Less
than half, 13 of those persons, report not having been diagnosed with asthma
and do not report having coughs that last more than 2 weeks. Data on respiratory
problems lasting more than one month are only available for primary respondents.
However, data on coughs and sore throats lasting more than two weeks was
available for both primary and other household members. A total of 165
people reportedly have coughs and/or sore throats lasting more than two
weeks. 6.7% (28) of the households have multiple cases of this ailment
going on. So, in addition to having 167 diagnosed cases of asthma in the
sample, we have 165 people with reported coughs and sore throats that last
more than two weeks. Ninety-five households (22.9%) of all households have
one case of cough/sore throat lasting more than two weeks. Twenty eight
additional households (6.7%) contain 42.4% of all cough/sore throats lasting
more than 2 weeks.
Allergies
One hundred and eighty five
persons in 149 households reportedly have allergies. Twenty seven of those
households have multiple allergy victims. One hundred and twenty two households
have a single victim. Allergies are even more concentrated in certain households.
Twenty seven households (6.5%) hold 34% of all allergy victims, while 29
households contain the other 66% of all allergy victims.
Table
2: Total Allergies in Household
| Frequency | Percent | Valid Percent | Cumulative Percent | ||
| Valid | .00 | 263 | 63.4 | 63.8 | 63.8 |
| 1.00 | 122 | 29.4 | 29.6 | 93.4 | |
| 2.00 | 22 | 5.3 | 5.3 | 98.8 | |
| 3.00 | 3 | .7 | .7 | 99.5 | |
| 4.00 | 1 | .2 | .2 | 99.8 | |
| 6.00 | 1 | .2 | .2 | 100.0 | |
| Total | 412 | 99.3 | 100.0 | ||
| Missing | System | 3 | .7 | ||
| Total | 415 | 100.0 |
Correlation and Regression Analysis
The apparent clustering of
these maladies in certain households strongly suggests that not all demographic
groups share equally in their distribution. Bivariate correlation analysis
yields results which strongly suggest that these ailments are being borne
disproportionately by Hartford's Hispanic population.
For both primary respondents
and other family members, there is a statistically significant relationship
between Hispanic status and increases in the incidence of asthma as well
as coughs and sore throats lasting more than two weeks. For respiratory
problems lasting more than one month, the relationship between race and
incidence amongst primary respondents is also statistically significant.
All of these relationships are significant at the .05 level or better.
Hispanics are between 1.5 and 3 times more likely than other demographic
groups to have asthma, coughs and/or sore throats lasting more than 1 week
and, for primary respondents, Hispanics are more likely to have respiratory
problems lasting more than 1 month.
This pattern holds true with
multivariate regression analysis. For total asthma in households, the population
most at risk is Hispanic. Important contributing factors include the presence
in the household of other respiratory and allergy problems.
APPENDIX I: Maps and Bar Graphs
Click on the Map or Chart to see a Larger Version
Connecticut Coalition
for Environmental Justice
The
Connecticut Coalition for Environmental Justice is an organization that
was established in Hartford in the summer of 1997. It was formed in response
to community concerns about the siting of yet another fossil-fueled power
generator in South Hartford as a consequence of the closure of Connecticut's
nuclear power plants. Residents were concerned that this was the tenth
power generator to be situated next to a neighborhood that is 80% Black
and Latino and that this neighborhood is already overburdened with significant
sources of air pollution, and its denizens suffer accordingly. CCEJ researched
the issue, raised public awareness about the relationship between air pollution
and respiratory health, requested a public hearing, and arranged the first
environmental public information session sponsored by competing neighborhood
groups. This was a highly successful strategy that led to an agreement
whereby
Northeast Utilities took the unprecedented step of removing the new power
generator.
Major
Accomplishments and Ongoing Activities
Since
that time, CCEJ has been active in many areas. In 1999, CCEJ's focus has
been to form, nurture, and staff the Hartford Environmental Justice Network
(HEJN). This first funded year of the Hartford Environmental Justice Network
has far exceeded our expectations. Our major accomplishments have been:
1.
Banning medical waste in Hartford.
Hartford is already home to more regional waste disposal facilities than
any other Connecticut town. It receives waste from 77 Connecticut towns,
Vermont, Massachusetts, Rhode Island, and New York City. Medwaste Management,
Inc. of New England proposed to add a ninth type of regional waste facility--a
medical waste treatment facility--to our overburdened city. Hartford Environmental
Justice Network was able to educate the community and policymakers to the
point that the Hartford City Council enacted legislation banning medical
waste storage and disposal in the City of Hartford.
2.
Sewage Sludge Compost Fire Accountability.
For more than eight days in November and December, one of Hartford's eight
regional waste disposal facilities--the MDC sewage sludge compost facility--burned
uncontrollably to the ground, thereby presenting an infectious disease
and air toxin hazard to nearby residents. HEJN hosted the only community
forum asking for an explanation of the cause of the fire, the response
of building, health and fire officials to the fire, and how to prevent
this from occurring at the other 7 regional waste facilities. Our efforts
led to an in-depth self-critical investigation of the fire by MDC.
3.
Protecting Coltsville Residents and Children.
We were able to get the state Department of Environmental Protection to
declare the former Colt's Firearm factory property to be a hazardous waste
storage facility. In addition, we were able to get the Headstart Program
moved off this contaminated site in June of 1999.
4.
Raised Awareness about the Relationship of Airborne Toxins From Incineration
of Trash and Asthma.
Now, a substantial portion of residents know about the large amount of
trash that we import to burn and the potential link with asthma. We have
persuaded the appropriate agencies to document asthma rates. This has lead
to the finding that, at 41 percent, Hartford has the highest documented
childhood asthma rate in the United States.
5.
Raised Environmental Concerns about the Cleanup of Adriaen's Landing.
HEJN members trained other residents to ask questions of the developers
to make sure that the contaminated site proposed for Adriaen's Landing
and the Patriots' Stadium is properly cleaned with a minimum of risk to
residents and workers before the project proceeds.
Environmental Background
Information Center (EBIC)
EBIC is a non-profit organization
which provides strategic research and assistance to community organizations.
We specialize in corporate, demographic and geographic research on conditions
and characters and other matters important to community groups.
EBIC s mission is to strengthen the advocacy and technical capacity of grassroots groups seeking to preserve, sustain and improve the quality of their environment and health and prevent the disproportionate burden of toxic pollution in poor and minority areas. We do this by providing information technology tools and other support that will assist local communities in making their voices heard, stopping harmful projects whose focus is on the bottom line rather than the community, holding corporate polluters accountable, facilitating networking and building power locally.
Appendix III: Correlation Matrices and Regression Tables
Race of Respondent * Has a physician
ever told you you have asthma
| Has a physician ever told you you have asthma | Total | ||||
| yes | no | ||||
| Race of Respondent | White | Count | 13 | 63 | 76 |
| % within Race of Respondent | 17.1% | 82.9% | 100.0% | ||
| Hispanic | Count | 36 | 70 | 106 | |
| % within Race of Respondent | 34.0% | 66.0% | 100.0% | ||
| Black | Count | 28 | 154 | 182 | |
| % within Race of Respondent | 15.4% | 84.6% | 100.0% | ||
| West Indian | Count | 7 | 29 | 36 | |
| % within Race of Respondent | 19.4% | 80.6% | 100.0% | ||
| Asian, American Indian, or Other | Count | 3 | 10 | 13 | |
| % within Race of Respondent | 23.1% | 76.9% | 100.0% | ||
| Total | Count | 87 | 326 | 413 |
Chi-Square
Tests
| Value | df | Asymp. Sig. (2-sided) | |
| Pearson Chi-Square | 14.941 | 4 | .005 |
| N of Valid Cases | 413 |
Race
of Respondent * Do you get a cough or soar throat lasting longer than two
weeks
| Do you get a cough or soar throat lasting longer than two weeks | Total | ||||
| yes | no | ||||
| Race of Respondent | White | Count | 14 | 62 | 76 |
| % within Race of Respondent | 18.4% | 81.6% | 100.0% | ||
| Hispanic | Count | 39 | 67 | 106 | |
| % within Race of Respondent | 36.8% | 63.2% | 100.0% | ||
| Black | Count | 28 | 153 | 181 | |
| % within Race of Respondent | 15.5% | 84.5% | 100.0% | ||
| West Indian | Count | 2 | 34 | 36 | |
| % within Race of Respondent | 5.6% | 94.4% | 100.0% | ||
| Asian, American Indian, or Other | Count | 4 | 9 | 13 | |
| % within Race of Respondent | 30.8% | 69.2% | 100.0% | ||
| Total | Count | 87 | 325 | 412 |
Chi-Square
Tests
| Value | df | Asymp. Sig. (2-sided) | |
| Pearson Chi-Square | 25.394 | 4 | .000 |
| N of Valid Cases | 412 |
Appendix IV: Miscellaneous
From Dr. Ellen Cromley
Dear Mr. Lipsett, I am sending
the corrected shape file (I moved the two points to the correct locations).
You will need all of the files I'm sending. If there is a problem, let
me know.
The file that I am sending
is Connecticut Coordinate System State Plane Coordinates, NAD-27, Clark
spheroid. The map units are feet.
The parcel boundaries and
annotation of building numbers and so on are in ArcInfo coverage format.
These are also NAD-27, etc.
I think it would be best
for you to handle all of the conversions to lat/lon, if that is what you
wish. All of DEP's data and data for the Metropolitan District Commission
(they prepared the building footprints, parcel boundaries, etc.) are projected
data. This is what was supplied to Mark Mitchell. If you wish to work with
the data in some other projection or unprojected, it would be best for
you to put the data into that format. Mark Mitchell has all of these data.
Also,the MAGIC website at the University of Connecticut is a source for digital geospatial data for all of the towns of Connecticut. You can download data for Hartford (1990 census tracts, and a lot of other data) in ESRI exchange (.e00) format, unzip the data, and bring it into
ArcView. These data are projected.
The URL is http:\magic.lib.uconn.edu.
From Arcview
The State Plane Coordinate
System was originally designed to use the North American Datum of 1927,
or NAD27. It uses the Clarke spheroid of 1866 to represent the shape of
the earth. The origin of this datum is a point on the earth referred to
as Meades Ranch in Kansas. Many NAD27 control points were calculated from
observations taken in the 1800s. These calculations were done manually
and in sections over many years. Therefore, errors varied from station
to station. To use one of the State Plane projections in NAD27, select
State Plane - 1927 from Projection Properties.